



If you are considering bariatric surgery, one of the most important decisions is choosing the procedure that best suits your individual health needs and weight loss goals.
The three most commonly performed bariatric procedures are:
All three procedures have been shown to help people achieve significant and sustained weight loss while improving obesity-related conditions such as type 2 diabetes, high blood pressure and obstructive sleep apnoea. However, they work differently and each has its own advantages and considerations.
The most appropriate procedure depends on many individual factors, including your medical history, existing health conditions, eating habits, nutritional status, lifestyle and long-term treatment goals. A comprehensive assessment by an experienced bariatric surgeon is essential before deciding which operation is most suitable.
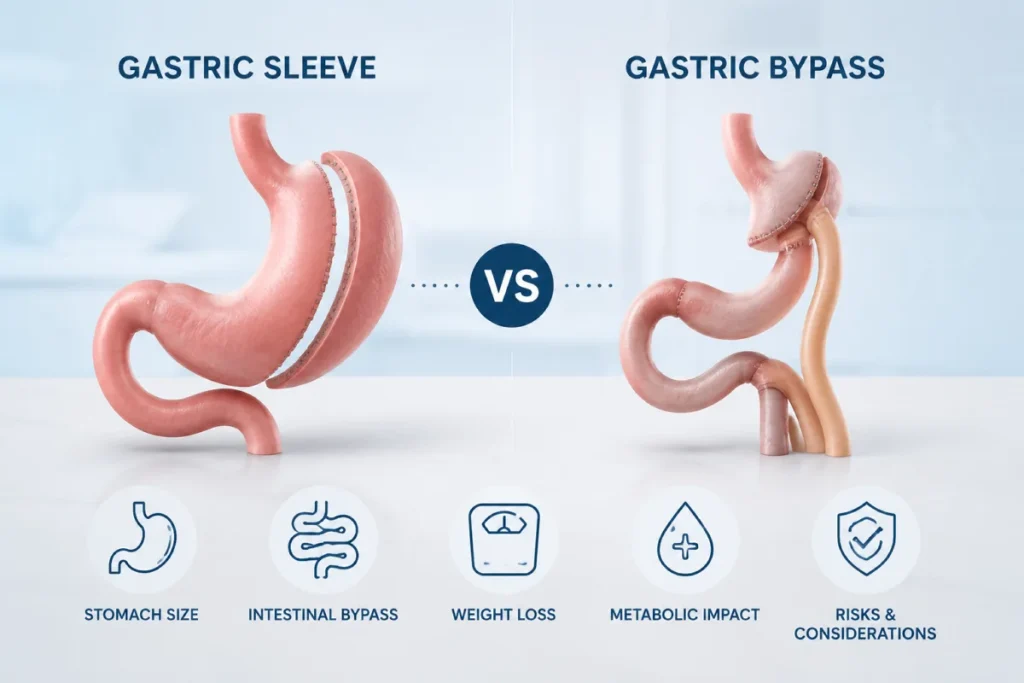
What Is the Difference Between Gastric Sleeve and Gastric Bypass?
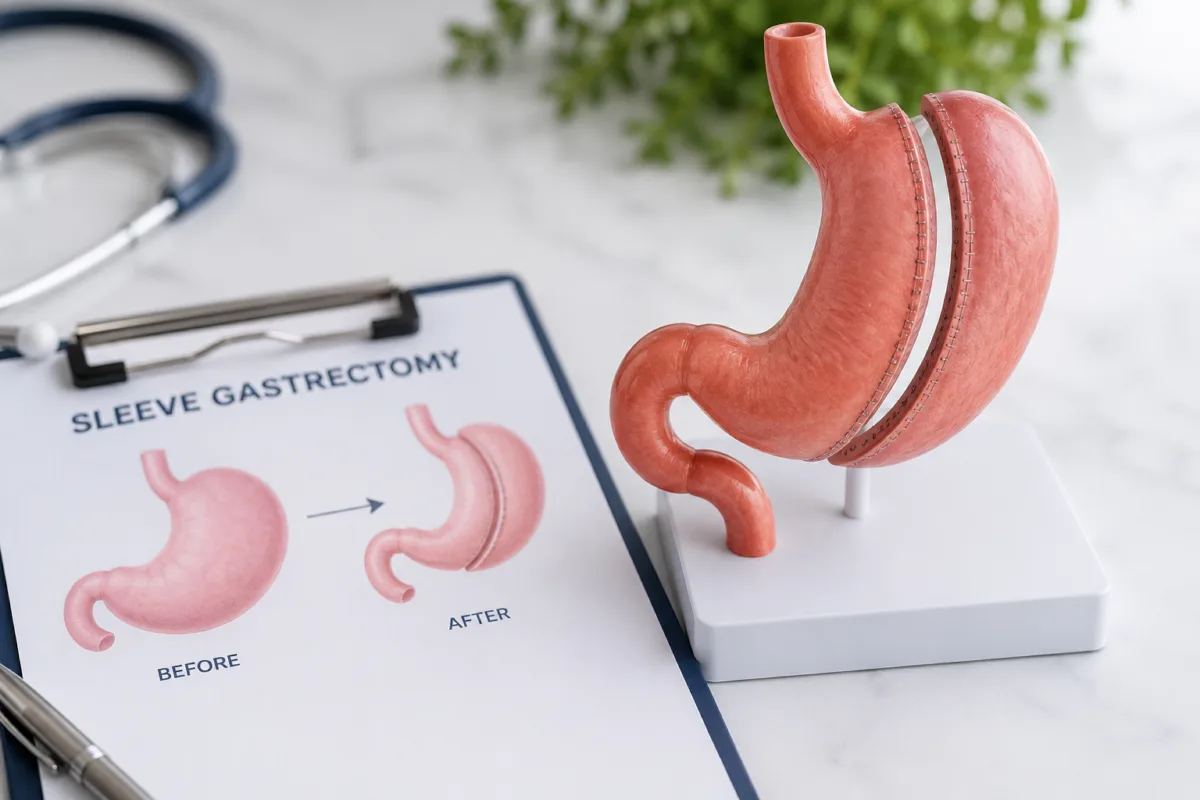
Sleeve Gastrectomy
A sleeve gastrectomy involves removing approximately 75–80% of the stomach, leaving a narrow tube or “sleeve.”
The operation works by:
- reducing the amount of food the stomach can hold
- decreasing production of the hunger hormone ghrelin
- improving hormones involved in blood sugar control and appetite regulation
The intestines are not bypassed, so food follows its normal digestive pathway.
Gastric Bypass
Gastric bypass procedures make the stomach smaller and reroute part of the small intestine.
This means they work through several mechanisms:
- restricting food intake
- altering gut hormones that regulate appetite and metabolism
- reducing absorption of some calories and nutrients
There are two commonly performed gastric bypass procedures:
- Roux-en-Y Gastric Bypass (RYGB)
- One Anastomosis Gastric Bypass (OAGB), also known as Mini Gastric Bypass
Although both procedures achieve similar goals, they differ in their surgical technique and long-term considerations.
Gastric Sleeve vs Gastric Bypass Comparison
| Feature | Sleeve Gastrectomy | Roux-en-Y Gastric Bypass | One Anastomosis Gastric Bypass (OAGB) |
|---|---|---|---|
| Stomach size | Approximately 75–80% removed | Small stomach pouch created | Long narrow stomach pouch created |
| Intestinal bypass | No | Yes | Yes |
| Number of bowel connections | None | Two | One |
| Mechanism | Restriction and hormonal changes | Restriction, hormonal changes and moderate malabsorption | Restriction, hormonal changes and moderate malabsorption |
| Weight loss | Excellent | Excellent | Excellent |
| Type 2 diabetes | Significant improvement | Often greater remission rates | Often excellent remission rates |
| Acid reflux (GERD) | May worsen or develop | Usually improves | May improve in some patients but carries a small risk of bile reflux |
| Nutritional deficiencies | Lower risk | Moderate risk | Moderate to higher risk |
| Lifelong vitamin supplements | Required | Essential | Essential |
| Technical complexity | Least complex | Most complex | Intermediate |
| Operating time | Usually shortest | Usually longest | Usually shorter than RYGB |
| Internal hernia risk | Very low | Higher | Lower than RYGB |
| Reversible | No | Difficult but possible in selected cases | Can be revised or converted if necessary |
When Might a Sleeve Gastrectomy Be Recommended?
Sleeve gastrectomy may be an appropriate option for people who:
- prefer a procedure without intestinal bypass
- have no significant gastro-oesophageal reflux disease (GERD)
- wish to minimise the risk of long-term nutritional deficiencies
- are suitable for a technically simpler operation
Although the intestine is not bypassed, lifelong dietary changes, vitamin supplementation and regular follow-up remain essential after surgery.
When Might Gastric Bypass Be Recommended?
Both Roux-en-Y Gastric Bypass and OAGB may be recommended for selected patients, particularly those with:
- poorly controlled type 2 diabetes
- severe obesity
- previous unsuccessful bariatric surgery
- specific metabolic conditions
Roux-en-Y Gastric Bypass is often preferred for patients with significant acid reflux because it usually improves GERD symptoms.
OAGB is technically simpler than Roux-en-Y Gastric Bypass because only one bowel connection is created, although it carries a small risk of bile reflux and requires careful lifelong nutritional monitoring.
Which Procedure Leads to Better Weight Loss?
On average:
- Gastric bypass procedures may achieve slightly greater long-term weight loss than sleeve gastrectomy.
- Gastric bypass procedures often produce greater improvement or remission of type 2 diabetes.
- Sleeve gastrectomy generally has a lower risk of nutritional deficiencies.
- Roux-en-Y Gastric Bypass is usually the preferred option for patients with significant GERD.
- OAGB provides excellent weight loss and metabolic outcomes but requires careful patient selection because of the potential risk of bile reflux and nutritional deficiencies.
The most suitable operation depends on your individual circumstances rather than one procedure being universally superior.
What Are the Risks and Long-Term Considerations?
All bariatric procedures require lifelong commitment to healthy eating, regular physical activity and ongoing medical follow-up.
Long-term care typically includes:
- lifelong vitamin and mineral supplementation
- regular blood tests to monitor nutritional status
- dietary review with an experienced dietitian
- routine follow-up with your bariatric team
- monitoring for weight regain or nutritional deficiencies
- ongoing management of obesity-related medical conditions
Long-term follow-up plays an important role in maintaining weight loss and supporting overall health after surgery.
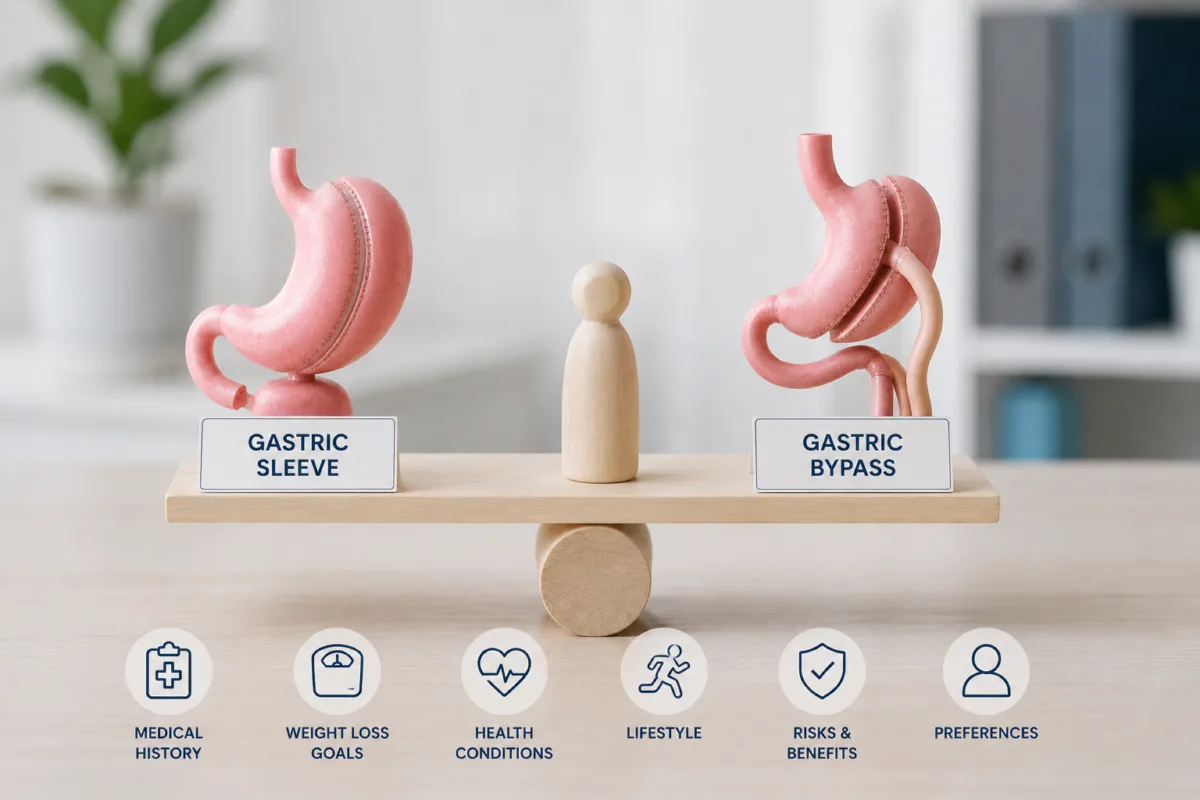
How Do Patients Decide Between Procedures?
Choosing between Sleeve Gastrectomy, Roux-en-Y Gastric Bypass and OAGB is based on a comprehensive assessment rather than simply selecting the operation with the greatest weight loss.
Factors that influence decision-making include:
- Body Mass Index (BMI)
- Type 2 diabetes and other metabolic conditions
- Acid reflux (GERD)
- Previous abdominal surgery
- Nutritional status
- Eating behaviours
- Future pregnancy plans
- Individual preferences and lifestyle
- Long-term follow-up requirements
An experienced bariatric surgeon will discuss the benefits and considerations of each procedure and recommend the option most appropriate for your individual circumstances.
Every patient is different. Dr Mani Niazi and the MBSA team can assess your individual health profile and guide you towards the bariatric procedure that best fits your needs and long-term goals.
Book a consultation